When the bone drug Prolia (denosumab) first came out in 2010, I took a hard look at it because it used a completely different mechanism than widely used bisphosphonate drugs, focusing on the RANK/RANK-L/OPG system to prevent osteoclasts from being “activated” instead of decreasing their number like bisphosphonates. I wasn’t satisfied in 2010 that this drug was any safer or more effective than bisphosphonates, and sad to say my skepticism has been borne out by recent research.
Dr. Brown’s 2024 Update:
Is Prolia a blockbuster bone drug — or a bust?
The FREEDOM Trial, which studied Prolia use in postmenopausal women for 3 years, found very little reduction in fracture risk. Vertebral and hip fractures were reduced 4.8% and 0.3% — meaning for 100 women they treated, only 5 saw fewer vertebral fractures than you’d expect with a placebo, and not even one woman was spared from a hip fracture by the drug. Given that hip fractures are considerably more harmful than vertebral fractures, these are minimal benefits indeed.
Although gains in bone density were observed, those gains were lost within 1 year of halting the drug (Cummings et al., 2017).
Furthermore, once they stopped using Prolia, patients’ risk of vertebral fracture quickly (<1–2 years) reverted to the same risk seen in those who’d never taken the drug in the first place (Cummings et al., 2017). They also lost a significant amount of the bone they’d gained by using Prolia — 35.5% of the total gain in the spine, 44.6% of the total gain in the femoral neck and 103.3% in the total hip (Zanchetta et al., 2017). In other words, the drug offered no lasting benefit.
Much more concerning: the finding that patients were more susceptible to having multiple vertebral fractures after discontinuing Prolia than patients who’d never taken the drug at all — and it was especially high in those who’d had such fractures prior to going on the drug in the first place (Cummings et al., 2017; Anastasilakis et al., 2017). This finding confirmed a number of earlier case reports of “rebound fractures” in patients who had discontinued Prolia within the preceding 12 months. Researchers speculated such fractures were a consequence of sudden renewal of bone resorption after the drug was stopped in combination with the absence of repair mechanisms during its use (Anastasilakis et al., 2017; Lamy et al., 2017; Polyzos & Terpos, 2016).
I’ve said repeatedly that working against nature invites unintended consequences, so I’m not surprised by these results. What is disappointing is the continued emphasis on the “magic bullet” approach to osteoporosis, when it has been clear for so many years that Proliajust doesn’t work.
Forteo™ (teriparatide) is a new and different drug on the scene as a treatment for osteoporosis. Other bone drugs, like Fosamax, Actonel, Boniva or even estrogen work to halt bone breakdown. Forteo, on the other hand, works to increase new bone formation. Short-term studies, in fact, report a common 9% increase in lumbar spine bone density and a 2–3% increase in hip density accompanied by significant reductions in fracture incidence. Sound too good to be true? Sure does. So let’s take a second look and try to understand this new drug from what the manufacturer, Eli Lilly, tells us in their 2008 Forteo Product Monograph.
What exactly is Forteo?
Forteo is a man-made (well, E. coli-made) recombinant parathyroid hormone that has an amino acid sequence identical to part of the human parathyroid hormone (PTH). Forteo was approved by the US FDA in 2001 as an osteoporosis drug.
How does Forteo work?
In the body, natural parathyroid hormone serves to regulate bone metabolism in many ways. Chronic elevation of PTH, as in hyperparathyroidism, results in increased bone breakdown, a loss of calcium and osteoporosis. On the other hand, daily injections of the PTH drug Forteo have the paradoxical effect of increasing bone mass and reducing osteoporosis. As scientists report, it seems to be that the pattern of exposure to parathyroid hormone determines its effect on the skeleton.
Through activation of various bone metabolic pathways, the PTH drug (Forteo) increases the number of active osteoblasts (bone-building cells), decreases the naturally programmed death of osteoblast cells and recruits bone-lining cells as osteoblasts. This drug appears to act largely upon the bone-building osteoblast cells stimulating them to overactivity. Safety studies on this drug in rats, in fact, have shown findings of excessive new bone formation and bone cancer. Interestingly enough, the cancer this drug was found to cause in rat studies (osteosarcoma — I’ll say a little more about this shortly) is a cancer often associated with high osteoblast activity and rapid bone growth.
By how much does Forteo reduce fractures?
Reduction of spinal fractures — Among 1,637 postmenopausal women with severe osteoporosis and one or more vertebral fractures at baseline, the drug produced a 9.3% absolute fracture risk reduction over 19 months.
Reduction of hip, pelvis, wrist, rib, humerus and other fractures — Over 19 months in these same high risk women, Forteo reduced nonvertebral fractures by an absolute 2.9% reduction in fractures.
So, overall, the short-term studies on Forteo reported above show this drug to reduce fracture risk substantially more than the bisphosphonate drugs like Fosamax. In addition, Forteo in these studies increased bone density more than the bisphosphonates.
Just how much does Forteo increase bone density?
In this same 19-month study of high risk osteoporotic women, Forteo increased bone density by an average 9.7% in the spine and 2.6% in total hip, while the wrist lost bone density and total body mineral content remained the same.
Why are there just short-term studies on Forteo, and is it safe?
As the manufacturer reports, the longest studies on the safety and efficacy of Forteo were of only a two-year duration. Why are there only short-term studies on this new drug? There are only short-term studies because in the animal safety studies, Forteo was shown to cause a high incidence of osteosarcoma (a rare malignant, often fatal, bone tumor), as well as osteoblastoma (abnormal mass of tissue in bone) and osteoma (small benign bone lesions). As with all drug safety tests, the drug doses tested were from 3-, 20-, and at times, 60-fold higher than those used in human medications. Notably, bone tumors were observed at all Forteo doses, with the incidence reaching 40–50% in the higher-dose groups.
Given this major safety concern, human trials with this drug were terminated early and guidelines were set to limit the duration of its use in humans. In fact, as the manufacturer specifically states, “The safety and efficacy of Forteo have not been evaluated beyond two years (median 19 months in women and 10 months in men). Consequently, the maximum lifetime exposure to Forteo for an individual patient is 18 months.” Also, given the cancer-causing effect of the drug, the FDA required a “black box” label warning, clearly stating the increased cancer risk shown in rat studies.
Expensive, experimental, possibly cancer-causing and inconvenient
As near as I can calculate, since its development, studies on this drug have included only 1,943 patients. According to the manufacturer, a study of one year is considered “long term,” while the maximum length of any study was only two years. Thus, not only is Forteo relatively new, but it is also experimental and, I would say, inadequately tested. In addition, it is very expensive — the drug costs upwards of $600–$700 per month! Further, it is inconvenient to use as it must be given as a daily self-administered injection. Most importantly, since this drug has shown to cause cancer in rat safety studies, its use by humans is limited to two years or less. While there may be significant bone density gains while using Forteo, the research is clear that these gains are lost once the drug is stopped. To maintain bone density gains, antiresorptive drugs such as Fosamax must be used after stopping Forteo.
Is there a better way?
This is the question I constantly ask myself — is there a better way to increase bone strength and reduce needless osteoporotic fractures? Is there a way that does not run the risk of causing cancer, or lead to excessive new bone formation — a way that is not only safe, but also good for the entire body? Yes, in most cases there is another way, and that way is through a comprehensive, life-supporting bone-building program that enlivens natural human healing and the body’s regenerative capacity.
In my previous two blogs, I’ve given you 4 important reasons why I don’t believe standard osteoporosis treatment is effective. In this final blog of the series, I want to emphasize that there is no magic bullet for optimal bone health – despite what you may have heard about calcium or bone drugs. Here’s why:
5. The calcium-centered focus has distracted us from the fact that at least 20 nutrients are essential for bone health
I’ve pointed out that calcium doesn’t reduce fracture risk and excessive calcium intake holds increased risk of cardiac problems. But if calcium isn’t the “magic bullet” for bones, what is? Well for one thing, adequate vitamin D levels are essential, and a lot of doctors are finally realizing how important vitamin D is for bone health.
Yet too little attention is still paid to other essential bone nutrients — especially vitamin K, which makes a major contribution to bone health and supports many other systems as well, but also zinc, magnesium copper, boron, folate, manganese and vitamin C.
6. Bone drugs are far less effective and far more risky than commonly thought
Here’s where it really becomes frustrating. Our health system pushes high-dose calcium (which doesn’t work) as the solution to low bone density (which is not necessarily the problem). Then when there’s no improvement in bone density from overloading the body with calcium, the typical next step is to prescribe a bone drug.
I’ve always maintained that such medications should be used only as a last resort, for very severe cases where drastic measures are needed — for instance, a person experiencing low-impact fractures or excessive, uncontrollable bone loss. This is not the situation for most people who have relatively low bone density .
With that in mind, it shouldn’t be surprising that the results of bone drug therapy are often very disappointing. Even worse, the evidence suggests no benefit from bisphosphonate bone drugs on real-world hip fracture incidence. Nor do these drugs benefit people 80 years old and older — which is, of course, the group most likely to fracture a hip!
What it all boils down to is this: If we’re to really help people to live long, healthy lives free from the fear of bone fractures, we don’t need more bone drugs. Instead, we need to change our approach by:
Carefully assessing each individual case to identify whether excessive bone loss or weakness exists;
Detecting and correcting both obvious and hidden causes of excessive bone weakening;
Broad-spectrum, whole-body support with nutrition, exercise, neuroendocrine and hormonal balance, stress reduction, and resilience enhancement.
Such an approach would limit bone drugs to the few specific situations where obvious bone weakness cannot be offset by natural means and requires heavy-duty intervention.
* Information presented here is not intended to cure, diagnose, prevent or treat any health concerns or condition, nor is it to serve as a substitute professional medical care.
I’ve written recently about two of my top six concerns about the standard approach to bone health. And now, here are two more that emphasize how women are often being misled about how to best protect their bones:
3. Contemporary osteoporosis management treats bone as if it were separate and isolated from the rest of the body
It’s tempting to look at the body the way we look at cars — as a collection of independent parts, each with a specific job. But that’s not what the body is! It’s a set of dynamic, interconnected systems that are constantly changing in response to what goes on around us and inside us.
While most people lose some bone as they age, bones don’t just “wear out” over time, the way a car’s parts do. If bones are weak or rapidly become thin, it’s nearly always because of a larger systemic problem in the body. The most effective approach in this situation is a big-picture perspective that looks at bone health as an indicator of overall health — it’s been shown that older adults who experience a hip fracture have lower baseline health-related quality of life than those who don’t.
But the standard approach is to focus on the mechanics of bone breakdown and interfere with them. Most bone drugs work by targeting the cells that break bone down and stopping them from doing their job. Doing this doesn’t actually solve the problem — it just masks the effects.
Enduring bone health requires rebuilding strength and vitality. That’s why it makes sense to look at the complete body system — circulation, bone, acid-base balance — to find the places where something isn’t working right to cause bone loss, rather than focus in on halting bone loss itself, which is most often an effect of a larger problem.
4. High-dose calcium is still considered the first-line treatment, yet it does not prevent fracture, and may be harmful
Speaking of “larger problems,” let’s take a look at what happens when you try to address fracture risk with calcium supplements. There is tremendous controversy about calcium and bones, but now it’s becoming clear that high-dose calcium supplementation is not the solution.
Multiple studies show that calcium does not decrease fracture risk except in those with a very low calcium intake — and some studies suggest that taking high-dose calcium supplements can lead to an increase in arterial calcification, stroke, kidney stones. In my own research, it’s quite clear that while adequate calcium is needed for healthy bones, using high doses is counterproductive.
It seems wise to obtain the total 1,200 milligrams of calcium daily from diet and supplements as recommended by the National Institute of Health. At the same time, we recommend you also learn about the other key bone nutrients and make sure you obtain adequate doses of all these essential bone builders.
Stay tuned for next week’s blog for my final two reasons the standard approach to bone health doesn’t make sense. And as you’ll see, are far less effective and far more risky than commonly thought!
Bolland MJ, Leung W, Tai V, Bastin S, Gamble GD, Grey A, Reid IR. Calcium intake and risk of fracture: systematic review. BMJ. 2015;351:h4580. doi: 10.1136/bmj.h4580. Bolland MJ, Grey A, Reid IR. Calcium supplements and cardiovascular risk: 5 years on. Ther Adv Drug Saf. 2013 Oct;4(5):199-210. doi: 10.1177/2042098613499790 https://ods.od.nih.gov/factsheets/Calcium-Consumer/
* Information presented here is not intended to cure, diagnose, prevent or treat any health concerns or condition, nor is it to serve as a substitute professional medical care.
It’s no secret that I’m not a fan of the way bone drugs like Prolia® and Fosamax® are used these days. But people sometimes misinterpret my thinking as being “anti-drug” — yet it’s not just the drugs I object to. It’s how medicine in general approaches bone health and fracture risk.
I have at least 6 major objections to the standard approach, but for the sake of brevity, we’ll look at them two at a time over the next three weeks.
1. Treatment is based on bone mineral density — but bone mineral density does not predict fracture
Having a low-side bone density isn’t actually a health problem. It doesn’t hurt or limit mobility — it doesn’t even necessarily mean the bones aren’t strong! It’s only when you fracture a bone that you have a health problem — and more, you cannot predict fracture by bone density alone. In fact, the majority of people whose bones are so fragile they experience a low-trauma fracture do not have an “osteoporotic” bone density.
That’s why treating low bone density bones as a “disorder” that “needs to be addressed” with heavy-duty medications makes no sense. Weak bones, on the other hand, need intervention. And, as far as weak bones go, there’s almost always an underlying problem causing the depletion of bone strength — whether it be nutritional, hormonal, bone-damaging medications, or some other hidden health condition or lifestyle factor. Properly detected and corrected these underlying causes can greatly reduce the risk of fracture. This is why a real fracture risk assessment and an assessment of underlying causes are so critical to developing a comprehensive bone-building program.
2. The standard medical approach to osteoporosis is fear-based — and fear actually damages bone
Given that a low-side bone density does not necessarily indicate weak bones, why do you suppose doctors are so adamant that people with a low-side bone density need treatment? They’re afraid their patient will have a serious fracture.
But fear of fractures is itself bone damaging and can be a self-fulfilling prophecy — literally, as studies have linked higher levels of stress and the stress hormone cortisol with osteoporosis and increased fracture risk. A recent Danish study, for example, showed that just the perception of stress — seeing yourself as stressed — increases risk of osteoporotic fracture by 68%. It is bad enough that we have so many reasons to fall into stress and worry, we really do not need our health professional piling on more stress with unfounded fears of fracture. Again, what’s needed is a fracture risk assessment leading to a comprehensive bone building program — one that includes stress reduction and hope.
It’s interesting to note that Traditional Chinese Medicine holds that bone health is determined by the “kidney energy” and that fear is the emotion that disrupts the kidney energetic system. (And even Western medicine links osteoporosis with renal disease because the kidneys play such a central role in vitamin D metabolism, mineral reabsorption, and acid-base balance. (As I have discussed before, when kidneys can’t adequately buffer metabolic acids, calcium from bones is called upon to rescue essential pH homeostasis.) The ancient Chinese wisdom tradition suggests that the kidneys control bone and fear damages the kidneys — and I have found this to be true. All in all, we need less fear and more hope and bone-building solutions.
Low-trauma bone fracture, rather than low bone density, is what indicates bone weakness — so if you’ve had a fracture, it’s a sign you need to take substantial, comprehensive steps to support your bones. Even a simple fracture of the wrist after stumbling tells a story — and what’s been shown over and over by research is that a person who’s had a previous fracture is at higher risk of future fractures (Johansson et al. 2017; Ferrari 2017; Gehlbach et al 2012).
Many international osteoporosis organizations have also reached this conclusion and have begun to recommend intervention after the first low-trauma fracture. The International Osteoporosis Foundation has developed the Europe-wide “Capture the Fracture” promotion, and Osteoporosis Canada a few years ago identified a significant post-fracture care gap. Both agencies, unfortunately, focus on moving fracture patients into a system of bone drug treatment.
5 steps to prevent a second fracture
At the Center for Better Bones, our approach to bone fracture prevention is fundamentally different. We view fractures that occur without high impact as very serious warning signs that are worthy of further investigation. We go about the goal of preventing a second fracture in a systematic fashion:
Step 1: Assess bone health
We guide individuals into assessing health and lifestyle factors that might be weakening their bones. A good way to begin this assessment is with our Bone Health Profile.
Step 2. Uncover causes of bone fragility
We encourage everyone who has fractured to ask their doctor for selected medical tests that help uncover hidden medical causes of bone fragility via a comprehensive osteoporosis work-up. The work-up offers direct data on possible health and lifestyle issues that may be contributing to your fracture risk.
Step 3. Address hidden medical issues
We review the results from your doctor’s medical testing, and if any hidden medical causes of bone weakening are uncovered, we help you understand them while your doctor treats these medical concerns.
Step 4. Reduce or eliminate fracture risk factors
We work with the client on the lifestyle and nutrition assessments to identify areas of lifestyle, diet, and emotional makeup that could be improved, with the goal of either eliminating these fracture risk factors or reducing their effects on your bones.
Step 5. Create a personalized plan for stronger bones
Based on our full assessment of the individual case and total load of fracture risk factors, we develop a personalized Better Bones, Better Body program to help modify lifestyle and nutritional factors and develop a strong nutrient supplement regimen to support stronger bones and reduce your future fracture risk.
Your bones are as unique as you are
In my experience, carefully evaluating each case and working with the body’s natural processes to regain optimal bone health offers far greater long-term benefits to health and longevity than any quick fix using bone drugs. This natural approach, however, requires a substantial level of commitment and a willingness to change one’s diet, lifestyle, and daily habits. As the old Chinese saying puts it: “If you keep going in the same direction, you will end up right where you are headed.”
There are undoubtedly extreme and severe case where bone drugs are deemed appropriate by both physician and patient, and in these cases, for optimum results we incorporate the complete Better Bones Better Body Program along with the bone drug.
So if you or someone you know has recently had a bone fracture, take heart — and take action! — to make this first fracture your only fracture.
Are you getting enough magnesium? The mineral may not immediately spring to mind when you think about important nutrients for your bones — but two new studies that found a strong relationship between insufficient magnesium and fracture risk could change this.
Low magnesium and hip fracture are connected
The first study (Kunutsor et al. 2017) found that having low magnesium levels in the blood correlated to a 44% higher risk of bone fractures, particularly hip fractures. This was done by looking at serum magnesium levels of 2,245 middle-aged men (age 43-61 years old).
The study noted that none of the men with what they regarded as “high” magnesium levels (more than 2.3 mg/dL) fractured at all. I should mention that the FDA sets the serum magnesium reference range at 1.8-3.6 mg/dL, so 2.3 mg/dL hardly qualifies as a “high” level of magnesium. It’s not even in the middle of the range! And that raises the possibility that chronic, latent magnesium deficiency may have been depleting the study participants’ bones of this needed mineral (Elin, 2011).
How much magnesium do you need to lower fracture risk?
Researchers also continue to reveal the importance of dietary intake of magnesium — especially for women. The second study (Veronese et al. 2017) included 1,577 and 2,071 women with an average age of 60 years. During the 8 year study, 560 participants — almost 15% — had a fracture. The risk of fracture also decreased significantly in the people who had the highest magnesium intake — 53% in the men, and 62% in the women.
One of the important findings was that in women, the effects were only seen to a significant degree in the ones who achieved the recommended daily allowance (RDA) of dietary magnesium, which was 320 mg/day (for men, it was 420 mg/day).
I generally recommend a daily magnesium intake of: 400-800 mg/day (which is somewhat higher than the RDA).
Here’s how to get the magnesium you need
I get two messages from these studies. One is obvious: We need to pay more attention to magnesium for healthy bones! Both studies show that people who lacked adequate magnesium would have benefited from having more, either through changes to their diet or by taking a magnesium supplement. They also show that even a small increase in daily magnesium intake can produce a significant effect. Ideally, though, we want to get enough to keep our bones healthy — and current ideas of what constitutes “enough” are probably too low.
The other message is perhaps less obvious, but no less important: chronic, latent magnesium deficiency is something you can probably fix pretty easily, assuming there’s no hidden disease process that prevents absorption. A good way to start is to try adding more magnesium-rich foods to your diet, like this easy salad recipe that gives you 350 mg of magnesium. You can also learn more about supplementing for magnesium with my Better Bones Basics.
Try this magnesium-rich warm salad
In a bowl, toss: 1 cup steamed or sautéed spinach (157 mg of magnesium) 1 avocado, sliced (58 mg of magnesium) 1/4 cup almonds (105 mg of magnesium) 3.5 ounces of sautéed tofu (30 of magnesium) Sea salt and pepper to taste (optional)
Hear Dr. Susan Brown talk about the importance of magnesium for bone health
References:
Elin RJ. Re-evaluation of the concept of chronic, latent, magnesium deficiency. Magnes Res 2011;24(4):225-227.
Food and Drug Administration. Investigations Operations Manual 2017: Appendix C. Silver Spring, MD: US FDA. Available at https://www.fda.gov/ICECI/inspections/IOM/ (accessed August 7, 2017).
It’s no secret that I’m no fan of bone drugs in general. I’ve found the arguments for their use deeply unconvincing for decades. And now, European researchers looking at the accumulated evidence about the various drugs’ long-term effects are starting to come to the same conclusion:
Except in extreme cases, bone drugs don’t offer enough benefit in reducing the risk of fractures to be worth the price paid in terms of both short- and long-term side effects.
A European/Canadian research group reviewed the evidence on bisphosphonates like:
alendronate (Fosamax),
ibandronate (Boniva) and zoledronic acid (Zometa or Reclast)
teriparatide (Forteo)
denosumab (Prolia)
two treatments not used in the U.S.: calcitonins and strontium ranelate
Their findings struck me as good general “lessons” for all of us to learn.
‘Denser’ bones are not always stronger bones
The review found that the majority of osteoporotic fractures happened in those who did not have “osteoporotic bone density.” This helps confirm: Bone density alone cannot predict fracture risk.
Other recent studies show a large percentage of people who fracture have only osteopenia or even normal bone density. Many people with an osteoporotic bone density never fracture.
Not all fractures are created equal
When it comes to assessing bone drugs’ effects, a painless vertebral fracture or a toe fracture (painful, but not life-altering) shouldn’t be considered as clinically important as a hip fracture, which is life-changing.
Yet many drug trials either focus on vertebral fractures or on “non-vertebral” fractures as an endpoint. The stubbed toe becomes equivalent to a hip fracture in determining how effective the drugs are in fracture prevention.
Not surprisingly, when hip fractures are looked at specifically as the endpoint of choice, the researchers discover something different. They found that the data on less serious fractures of toes, wrists and so forth obscure the fact that the drugs don’t do much to prevent the most serious and dangerous osteoporotic fractures.
Bone drugs’ benefits remain inconclusive
The benefits of taking a bone drug must outweigh the costs for it to be worth recommending. And even in high-risk older adults, such benefits have not been shown conclusively.
In weighing the risk-benefits of bone drugs, researchers took a hard line on the importance of evaluating all costs. “Clinical trials evaluating harm-benefit balance in osteoporosis or fracture prevention should be well-powered long-term studies that include hard endpoints,” they note. “Total mortality, total serious adverse events, hip fractures, and functional status are essential outcomes.”
New U.S. osteoporosis guidelines miss the mark
What’s frustrating to me is that experts in the U.S. still focus uncritically on the flawed studies that the review critiques. They glibly parrot the ideas that bone density is the same thing as fracture risk and that drugs offer protection from fractures.
Case in point: The American College of Physicians’ latest osteoporosis guidelines, which were published virtually simultaneously with the European review. They make a “strong recommendation” for the use of bisphosphonate drugs “to reduce the risk of hip and vertebral fractures.” Most galling to me, they openly equate bone mineral density with fracture risk: “most women with normal DXA scores” it notes, “do not progress to osteoporosis within 15 years.”
To which I respond with the European review’s first lesson: Denser bones ≠ stronger bones.
It’s an unusual person who gets to middle age without a few aches and pains — a little wear and tear is to be expected after a half century or so. But for those at risk of osteoporotic fractures, back pain is particularly worrisome because you can’t really know whether it’s tired muscles, or arthritis, or a vertebral fracture.
Or can you?
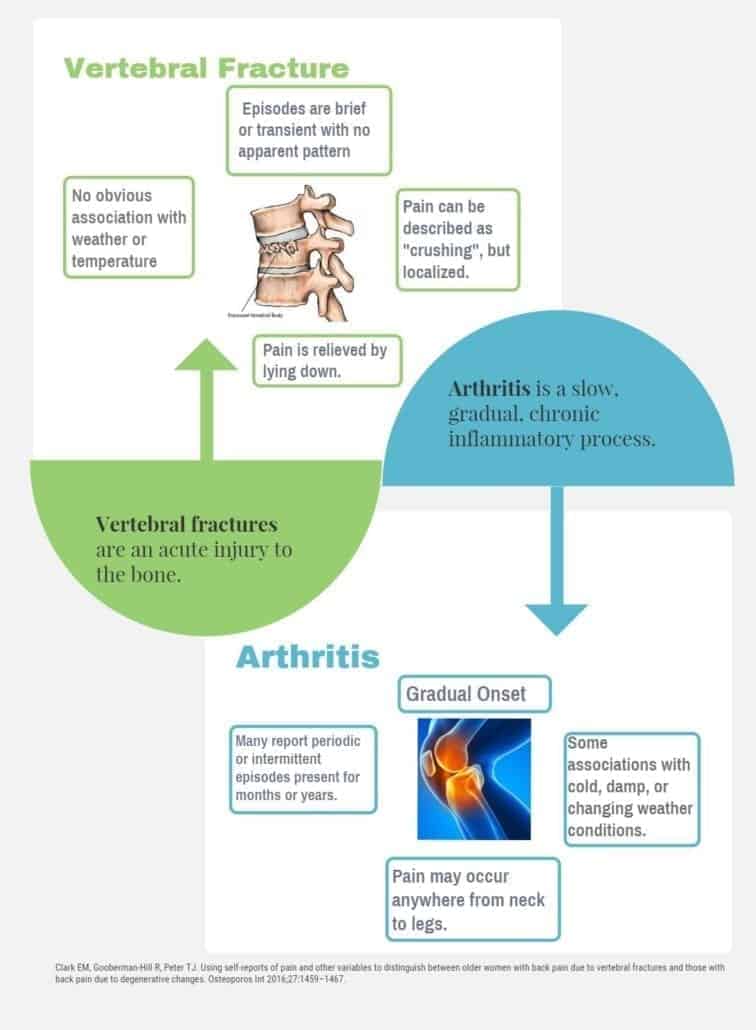
Recent research shows that the pain caused by vertebral fractures is different from other causes, such as arthritis of the spine. As a 2016 study published in Osteoporosis International found, vertebral fractures in women produced a number of distinct pain signposts that weren’t present in women who had arthritis of the spinal column.
Recognizing the signs
The study looked at 197 British women between the ages of 67 and 84, asking them to report on their experiences of pain (in the back but elsewhere as well) before initiating a spine x-ray to look for vertebral fractures. They found that about a third of the women had vertebral fractures — and the women with fractures had a number of things in common. They were older (average age of 76.9 years versus 71.7 in the women without fractures), were considerably more likely to have had a previous fracture, or a diagnosis of osteoporosis, or both, and had fairly specific attributes to the pain they experienced that differed from the women with arthritis.
Most notably, women with fractures described their pain as recent and brief in duration but “crushing,” whereas women with arthritis said they had intermittent or periodic pain that they were more likely to call “taut” or “sharp.” Radiation of pain to the legs and association with weather changes were common in the women with arthritis but not the women with vertebral fractures. (See table for full comparison.)
Table: Women’s experience of vertebral fracture pain
Vertebral fracture
Arthritis
Risk factors
Older age
Previous fracture (nonvertebral)
Diagnosis of osteoporosis
Duration of pain
Short-term, recent (occurring within days or weeks of the study); episodes are brief or transient with no apparent pattern
Long-term (present months or years prior to study); episodes are “periodic” or intermittent
Onset
Sudden
Gradual
Type of pain
“Crushing” but localized
Pain description varies but it is ongoing or intermittent and may occur anywhere from neck to legs
Other
Relieved by lying down
Does not radiate to legs
No obvious association to weather or temperature
No clear effect on pain of keeping still or moving
May radiate to legs
Some associations with cold, damp, or changing weather conditions
Listening to your body
All of this makes sense. Fractures are an acute injury in the bone, which is very different from the kind of slow, gradual, and chronic inflammatory process that is present in arthritis.
What I take away from this study is that our body will tell us what we need to know — if we listen carefully. To start learning more about your bone health and risk for fracture, I encourage you to take our quick and easy Bone Health Profile.
We are excited to announce this amazing opportunity to develop your own personalized Better Bones, Better Body program under the guidance of Dr. Susan Brown in an intimate group setting.
The Love Your Bones, Love Your Life retreat will get you started on the road to a healthier and more vibrant you. This retreat will be your pathway to self-empowerment, better bone health, renewed vitality, and overall wellness.
Now is the time to take action. No one cares about your health as much as YOU do!
The Details
This 4-day Better Bones, Better Body retreat and workshop covers everything you will need to manage and reverse your osteopenia or osteoporosis naturally! This includes a 1-hour new client consultation & support kit (a $575-value) before the retreat! Once you pay your deposit, you can book your consultation and get started. No need to wait until September to begin your natural bone-building program!
In this retreat we will learn... how to build bone naturally... how to reduce worry & fear... the best bone building exercises....about gourmet alkalizing food.... nutritional supplementation individualized for you how community can build bone!
When: Thursday, September 24th to Sunday September 27, 2020 (New Dates)
Where: Himalayan Institute, Honesdale, PA
Cost: $975 tuition* plus your choice of accommodations at the Himalayan Institute starting at $95/night including meals (must book separately).
*Tuition does not include travel expenses, lodging, or transportation to and from the Himalayan Institute.
Call us at 1-877-207-0232 for questions on room options or other retreat details.
Final Payment due by May 15, 2020.
Love Your Bones, Love Your Life Retreat Includes:
4 daysand3 nights in the lovely retreat center in Honesdale, Pennsylvania. Amenities at the retreat center include 400 acres of beautiful walking paths, a brand new meditation shrine, PureRejuv Wellness Center, a tea lounge, the Himalayan Gift Shop, and morning and evening yoga classes. Himalayan Institute has everything you need for relaxation and rejuvenation. Learn More.
Meals are provided Thursday evening through Sunday lunch and will consist of healthful vegetarian options with an emphasis on traditional Ayurvedic themes. Learn more.
Dailylecture sessions with Dr. Brown covering the 6 key steps of the Better Bones, Better Body® Program. You will leave these sessions with greater ability to implement or expand upon your Better Bones, Better Body® Program at home.
Every attendee will receive a one-hour preparatory consultation (included in tuition) with Dr. Susan Brown, PhD prior to attending the Love Your Bones Retreat. This will also include customized charting of your bone density tests and lab tests as well as personalized consultation notes with nutrient supplement protocol for the implementation of your Better Bones, Better Body® Program.
Afternoon exercise workshops with E-RYT 200, Gina Galli. Gina will be demonstrating safe yoga postures for strong bones as well as leading spine and hip strengthening workshops.
E-RYT 200 Gina Galli doing the Warrior Pose in front of beautiful red rock vistas in Sedona, AZ
Evening Q&A led by Dr. Brown where you can ask your most pressing questions!
Optional: Meditation before dinner led by Dr. Brown.
The Better Bones, Better Body program support kit mailed to you before the start of the course so you can begin “boning up” before the retreat.
Better Bones, Better Body® gift bag and course materials (over $100 value).
Supplements in the program will be available to try as well as supplement demos and one-on-one nutrient coaching with our client support team.
Not Included:
Travel & airfare, lodging, and transportation to and from the Himalayan Institute.
Additional one-on-one time with Dr. Susan Brown PhD during the retreat weekend.
Here are directions for getting to the Himalayan Institute.
See sample schedule below. (Full schedule will be mailed to program participants.)
See past attendees talk about their experiences at some of our other Love Your Bones, Love Your Life retreats.
Sample Schedule:
Arrive at Himalayan Institue, Honesdale, PA
Dinner @ 5:30 PM
Staff Introductions and Guest Sharing
Program Overview/How to Asses Your Case by Dr. Susan Brown PhD
Friday /Saturday
Breakfast
FRI — Alkaline Diet SAT — Bone Building Exercise Modalities
BREAK
FRI — Key Bone Building Nutrients SAT — Stress and Worry Reduction
Lunch
Exercise Workshops with Gina Galli – 12 Yoga Poses for Osteoporosis/Hip and Spine Exercises for Osteoporosis
BREAK/Optional Group Work and Scheduled Time with Dr. Brown and Assistants
Dinner
FRI — Digestion and Detoxification SAT — Bone Drugs
I was looking to the retreat but I have to say that it exceeded all of my expectations. The Mago Resort set the stage for a soulful experience. I felt so incredibly safe to share my situation and feelings with these wonderful women. The information provided, the yoga and gentle stretches, the meditative rituals all integrated together to provide such a sound mind body connection. The mantra that I found in the last circle holding hands was “I am Vibrant, I am Strong” Thank You Dr. brown for your incredible research and belief that there is a better way to gain bone strength. Loved having you sit with us at meals and sharing in everyday conversation. This experience has changed my life ~Sedona Attendee
It was so helpful to have the opportunity to come together with other women dealing with this health issue. Many times I have felt like I’m out there on my own dealing with with this. The support and sharing the retreat provided was priceless.
Truly grateful for the common sense approach/support/encouragement offered by Dr. Brown and her staff. Have felt frustrated and hopeless about bone loss but now feel that there are options. I came away feeling positive, energized, and ready to take action.
I was struck by the attention given to every detail, making the retreat so seamless, comfortable, and nourishing to mind, body, and spirit.
As far as the retreat format itself, I thought it was very well planned and had just the right mix of lectures, stretching/exercise sessions and optional activities. Location was ideal! I liked that there were samples of the supplements available to view and to try out. Also, I have a weight vest and really appreciated the demonstration so that I now better understand how to use it properly.
I’m so glad I found Dr. Brown’s website and signed up for the retreat. It was everything I had hoped it would be.
I am so grateful for the work Dr. Brown is doing to strengthen Women in so many ways. Bones- whole bodies- and Minds! Her enthusiasm for life is contagious! I look Forward to strengthening myself with all this information. One weighted step at a Time!
I appreciated
The research and client practice that provides us with a whole-health approach to bone health and an alternative to bone drugs;
The retreats to share information and build community (and to have fun in a beautiful place!); and
The sense of empowerment, support and hopefulness for improved bone health and general health I gained from the retreat.
I just want to add that this workshop has provided us with the tools to take control of our quest for healthy bones. Thank you, Dr. Brown and staff for this amazing gift.
I have just received my supplements and am so excited to get started after such an amazing retreat with all of you awesome women! I can’t thank you enough for the great information shared in Sedona. Every session was orchestrated perfectly…with all that personal, caring, compassionate touch. I feel hopeful, empowered and confident that I am on the right road to stronger bones! Also, I’m enjoying my weighted vest… up to 7 lbs. and walking a minimum of an hour. Thank you to all of you for spreading the joy of knowledge… it is truly powerful! I’m so grateful!