According to the National Osteoporosis Foundation, up to one-half of women age 50+ will experience a bone fracture during the remainder of their lifetime. This means a lot of women will fracture, so it’s important to familiarize yourself with the better-documented fracture risk factors. Over the years, researchers have tried to quantify how much any factor increases the risk of bone fracture.
Chart: Top 7 bone fracture risk factors
Look over the top 7 risk factors for bone fracture, ranked by risk ratio. This measure of “relative risk” represents the likelihood of a certain event happening in one group compared to the risk of the same event happening in another group.
Risk factor
Risk ratio
Glucocorticoids (steroids)
2.31
Parental hip fracture
2.27
Low BMI (20 vs. 25)
1.95
Rheumatoid arthritis
1.95
Prior fragility fracture
1.85
Current smoking
1.84
High alcohol intake
1.68
Are you concerned about risk factors that may be present in your life? Begin by assessing your personal health and lifestyle factors with our free Bone Health Profile. As we at the Center for Better Bones like to say, “It is never too late to begin building and rebuilding bone strength.”
The saying, “You can never be too rich or too thin” is definitely not true when it comes to bone health! It’s well established that women with low body weight have lower bone density and are at increased risk for many types of bone fracture.
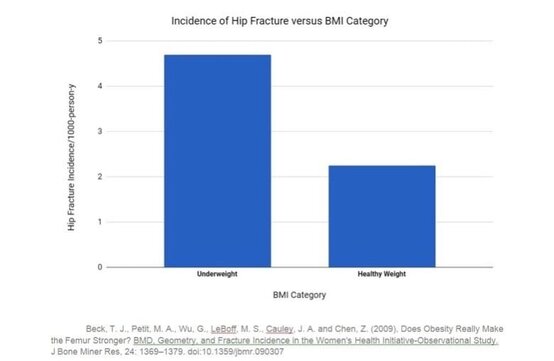
Experience twice the rate of hip fracture as do “healthy weight” women. (See chart below.)
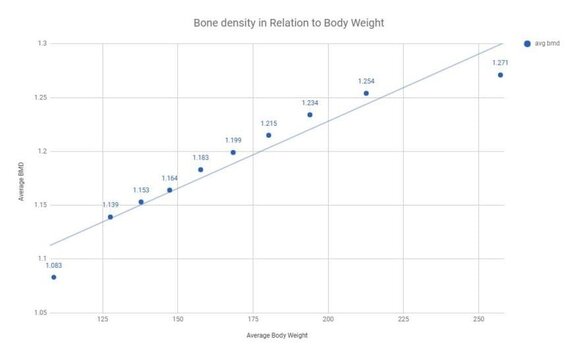
Have lower hip bone density, lower cross-sectional bone area, and less bone bending strength than “normal” weight women.
Experience more vertebral and wrist bone fractures (but fewer lower leg fractures).
Tend to lose more bone during the menopause transition than do heavier women.
So just who is included in this “underweight” category?
The “underweight” designation is determined by body mass index (BMI) using weight and height. A BMI of 18.5 or less (which would translate into a 5’3” women weighing 105 lbs or less, or a 5’5” person weighing 115 lbs or less) is considered underweight.
While the “underweight” category includes only very thin folks, there exists a weight–bone gradient link whereby lighter weight individuals have both decreased bone density and increased risk of various fractures. Those falling into the “underweight” category are at highest risk, but slender individuals (that is, those whose BMI is 18.6–21.5) are often reported to be at increased bone fracture risk, too, particularly if they also have low muscle mass.
How can underweight or slender women reduce their fracture risk?
This is indeed a complicated topic, which I can only begin to address here. As always, at the Center for Better Bones we look for the root cause of the problem and seek a solution with this in mind. Being significantly underweight likely indicates a serious imbalance within the system, such as digestive, emotional, or disease-related issues:
Low body weight is often associated with weak digestion, food allergies, or food intolerances. Addressing these issues is central to improving your metabolism. Check out our 10 steps to stronger digestion and try a simple elimination diet.
Clinically, I also see low body weight associated with a tendency towards anxiety, nervousness, and at times even straight out emotional distress and fear. While uprooting these negative emotional responses can take some time and good guidance, a good place to begin is with our free e-book, 7 secrets to reducing stress.
If you’re an “eat-and-run” person or you regularly skip meals, discipline yourself to sit down, relax, and consume three tasty, wholesome meals every day.
Try not to get extra calories from simple carbohydrates like sugars, pastas, and flours. Instead, increase your intake of root crops and wholesome fats like avocado, nuts, seeds, and olive oil.
As you can see, there’s a lot that a thin, small-framed person can do to strengthen bone and reduce their fracture risk. Being aware of your risk is the important first step!
Low-trauma bone fracture, rather than low bone density, is what indicates bone weakness — so if you’ve had a fracture, it’s a sign you need to take substantial, comprehensive steps to support your bones. Even a simple fracture of the wrist after stumbling tells a story — and what’s been shown over and over by research is that a person who’s had a previous fracture is at higher risk of future fractures (Johansson et al. 2017; Ferrari 2017; Gehlbach et al 2012).
Many international osteoporosis organizations have also reached this conclusion and have begun to recommend intervention after the first low-trauma fracture. The International Osteoporosis Foundation has developed the Europe-wide “Capture the Fracture” promotion, and Osteoporosis Canada a few years ago identified a significant post-fracture care gap. Both agencies, unfortunately, focus on moving fracture patients into a system of bone drug treatment.
5 steps to prevent a second fracture
At the Center for Better Bones, our approach to bone fracture prevention is fundamentally different. We view fractures that occur without high impact as very serious warning signs that are worthy of further investigation. We go about the goal of preventing a second fracture in a systematic fashion:
Step 1: Assess bone health
We guide individuals into assessing health and lifestyle factors that might be weakening their bones. A good way to begin this assessment is with our Bone Health Profile.
Step 2. Uncover causes of bone fragility
We encourage everyone who has fractured to ask their doctor for selected medical tests that help uncover hidden medical causes of bone fragility via a comprehensive osteoporosis work-up. The work-up offers direct data on possible health and lifestyle issues that may be contributing to your fracture risk.
Step 3. Address hidden medical issues
We review the results from your doctor’s medical testing, and if any hidden medical causes of bone weakening are uncovered, we help you understand them while your doctor treats these medical concerns.
Step 4. Reduce or eliminate fracture risk factors
We work with the client on the lifestyle and nutrition assessments to identify areas of lifestyle, diet, and emotional makeup that could be improved, with the goal of either eliminating these fracture risk factors or reducing their effects on your bones.
Step 5. Create a personalized plan for stronger bones
Based on our full assessment of the individual case and total load of fracture risk factors, we develop a personalized Better Bones, Better Body program to help modify lifestyle and nutritional factors and develop a strong nutrient supplement regimen to support stronger bones and reduce your future fracture risk.
Your bones are as unique as you are
In my experience, carefully evaluating each case and working with the body’s natural processes to regain optimal bone health offers far greater long-term benefits to health and longevity than any quick fix using bone drugs. This natural approach, however, requires a substantial level of commitment and a willingness to change one’s diet, lifestyle, and daily habits. As the old Chinese saying puts it: “If you keep going in the same direction, you will end up right where you are headed.”
There are undoubtedly extreme and severe case where bone drugs are deemed appropriate by both physician and patient, and in these cases, for optimum results we incorporate the complete Better Bones Better Body Program along with the bone drug.
So if you or someone you know has recently had a bone fracture, take heart — and take action! — to make this first fracture your only fracture.
How many of you have fallen and thrown out your hands to catch yourself? It’s probably happened to most us, and may be one reason that in the U.S., 1 in 10 broken bones is a broken wrist.
But wrist fractures aren’t just due to accidents. Wrist fractures that occur from a fall from standing height are generally a sign of bone weakness and are the most common osteoporotic fractures.
Having seen my grandmother experience first a wrist fracture, then a collarbone fracture, and finally a hip fracture, I suspected that wrist fractures — common in middle-aged and older women — are an important sign that attention should be given to strengthening bone.
Wrist fractures signal increased fracture risk
And there’s a recent study out that confirms this suspicion. In a 2015 study from the Journal of Bone and Mineral Research (Crandall et al., 2015), the study authors looked at long-term data from more than 160,000 women and found that women who’d previously had a wrist fracture were at significantly higher risk of other fractures during the almost 12 years of follow-up — regardless of other osteoporosis risk factors.
The big news . . . the younger the woman was when she fractured her wrist, the greater her relative risk of having another fracture later on.
I like to say, make your first fracture your last fracture. If you’ve fractured a wrist in the past, be aware that this fracture is your “canary in the coal mine” telling you to pay attention to your bones. You can take the Better Bones Profile to assess the health of your bones and your potential risk of fracture.
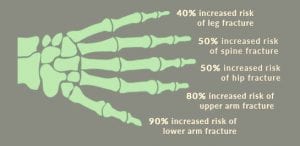
Are you taking medications that could increase your risk of osteoporotic fracture? Many people are – even after they’ve suffered a fracture – according to a recent article about osteoporotic fractures and medication use from the Journal of the American Medical Association (JAMA).
Scientists looked at 168,000 Medicare beneficiaries who experienced osteoporotic fractures of the hip, shoulder, or wrist. They found that 75% of these patients had actually been taking one or more medications known to increase fracture risk.
Drugs known to increase fracture risk
In the study, 21 classes of drugs were associated with increased fracture risk. Some of the drugs known to increase fracture risk include:
Glucocorticoid steroids (e.g., prednisone)
Serotonin re-uptake inhibitors (antidepressants)
Antacids (proton pump inhibitors and aluminum-containing antacids)
Blood pressure medicines
Antipsychotics
Thyroid hormone (when dosed in excess of need)
Anti-seizure medications
Anti-estrogen breast cancer drugs
Anti-testosterone prostate cancer drugs
DepoProvera
Sedatives (benzodiazepines)
Opiate pain killers, morphine
Acetaminophen if used long term
Diabetes medications (thiazolidinediones)
Heparin, long term use
What can you do to reduce your bone health risks from medications?
The authors of the study were struck by the fact that even after fracturing, patients did not stop using their bone-damaging medication. One obvious helpful suggestion from this study is for doctors to provide alternative medications that damage bone less. Here are other ideas for creating lifelong bone health:
When a drug therapy is recommended, dig a little deeper! Learn more about your health condition and how it’s related to lifestyle and nutrition.
Use the medication for the shortest period possible. When you need medication for a chronic condition, work with your doctor to minimize the dose or find a less bone-damaging alternative.
Study how others with this ailment have regained health using natural, life-supporting alternatives to drug therapy, including exercise, nutritional strategies, and methods that strengthen the mind–body connection.
Look into the more holistic health approaches, such as functional medicine, acupuncture and traditional Chinese medicine, classic homeopathy, chiropractic, and massage.
If you’re concerned about your risk for fracture and other bone health issues, take a moment to learn more about my natural Better Bones Program.
Getting enough fish oil daily in midlife is associated with lower fracture risk for women later in life, according to a major study from the University of Iceland. And when news about a significant decrease in fracture risk comes from researchers in a country where fracture risk is high, I certainly pay attention.
In the Icelandic study, women who got high daily amounts of polyunsaturated fatty acids from fish-oil consumption during midlife had a 25% lower risk of fracture compared to those who didn’t. The risk of fracture for men who consumed fish oil daily was even less – up to 45% less than those men who had lower levels. For men, getting optimal amounts of fish oil later in life was associated with lower fracture risk.
Are you getting enough omega-3s in your diet?
Closer to home, the average American only gets about 200 mg per day of the most important omega-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) from their diet. The American Heart Association recommends a much higher intake of between 1,000 and 3,000 mg. Test Your Omega 3 Level At Home!
Good omega-3 food sources
Omega-3s are found in a wide range of foods, including many fish sources. But vegetarians and vegans can also get omega-3s from food, with research showing a diet high in omega-3s from plant sources may be just as effective as those from fish sources. Here are my favorite choices for omega-3 rich foods:
• Seafood (sources both high in omega-3s and low in environmental contaminants include anchovies, herring, mackerel, oysters, wild salmon, and sardines) • Fresh ground flaxseed • Flaxseed oil • Hempseed oil • Canola oil • Avocados • Walnuts • Eggs • Pumpkin seeds • Sesame seeds • Olives
As it sometimes can be difficult to get the full amount of omega-3s from diet alone, many women choose a daily high-quality omega-3 supplement. I recommend Omega-3s that are molecularly distilled to help you get all of the key benefits for your bones, joints, immune system, heart, skin and more.
If you stop to think about it, maintaining our upright human posture on two legs is pretty tricky! Staying balanced requires instantaneous coordinated efforts from the brain, muscles, nervous system, ears, eyes and even the joints.
Most of us manage good balance effortlessly (for the most part) until we start to age. Then changes to our vision, ear canal issues, muscle loss and medication use can cause decline in our balance. Missteps come more easily, tripping is more common and recovery is more difficult. You might have noticed that walking on uneven ground is a bit more challenging, or that you are less stable walking in the dark.
All these are signals reminding us to tone up our balance, and the good news is that everyone can improve balance dramatically with just a few simple, mindful exercises. Cultivating good balance should be central to everyone’s bone health program. In fact, studies repeatedly show that balance improvement — through tai chi, yoga, strength training or simple balance exercises — even reduces fracture rates.
In the video below, our fitness expert Gina Galli and I demonstrate a few simple activities that can help you regain excellent balance right now. We also demonstrate a new Better Bones balance gadget that I really like — the OPTP Pro Balance Pad. Hope you enjoy our demo!
I’ve noticed that when I approach things from a little different angle I gain new insights. So, in celebration of May as “National Osteoporosis Awareness and Prevention Month,” let’s look at osteoporosis from a little different perspective than what many conventional practitioners tell us:
Did you know . . .?
Up to 80% of all those who experience an “osteoporotic” fracture do not have “osteoporosis” as defined by bone density (that is, a T-score of -2.5 or greater.)
Instead, they may have “osteopenia” or even normal bone density. These fractures are not related to mineral density issues, but to sub-optimal health and inadequate repair of the bone protein collagen matrix.
What this means for you: Get enough of all the 20 key bone nutrients daily as well as adequate protein to enhance healthy bone protein matrix.
You can reduce your real risk of fracture even without gains in bone density.
For example, supplementation with vitamin K2 strengthens bone and reduces fracture risk without substantially increasing bone density. Strength training also significantly reduces fracture risk yet only causes minor changes in bone mineral density.
What this means for you: Go beyond seeing bone density as the most important factor in bone health. Consider your total body muscle strength, balance, wellness, and zest for life. Keeping bone density loss to a minimum is important, but big gains are not essential for useful fracture reduction.
Bone size matters
Small and thin women have special bone health concerns. For example, small bones break more easily than larger ones; thin women lose more during the menopause transition; and often as a group they experience tendencies toward weak digestion, poor sleep, low energy, excess worry and anxiety, and low bone formation.
What this means for you: If you’re thin, much less thin and worried, keep building and maintaining bone strength as top priorities. Take care not to lose weight, since when you lose weight you also lose bone.
During the transition into menopause the average woman loses 10% of her bone mass
And many thin women and selected others lose up to 20%. Interestingly enough, much of this loss occurs in the first year before the last period.
What this means for you: Begin a bone building program well before you see signs of the menopausal transition. Bone loss actually begins in the early 30s. Even in youth we need to build stronger bones with appropriate diet, exercise, and nutritional supplementation.
Remember, it is never too late (nor too early) to build, and rebuild, bone. And what better time to start than National Osteoporosis Awareness and Prevention Month!
Awhile back I told you about early research connecting menopausal hot flashes to lower bone density and a higher rate of bone breakdown. These findings from Dr. Carolyn Crandall, MD made a lot of sense to me, especially given the inflammatory nature of both hot flashes and osteoporosis.
Now, the evidence of the connection between hot flashes/night sweats and bone health just got even more powerful, with new research from Dr. Crandall. In one of the first studies looking at how hot flashes and night sweats are related to fracture incidence, she found women who experience “moderate to severe” menopausal hot flashes or night sweats have almost double the risk of hip fracture in later life. The study was also a large one, including data from more than 23,000 women ages 50 to 79.
I believe this study adds to the urgency of taking care of your bones during menopause. We know that hormonal changes during menopause disrupt your body’s natural bone-building process. Your body may have less estrogen, which is needed to help preserve calcium in the body and prevent bone breakdown. The low progesterone levels common in perimenopause may also affect bone-building cells, disrupting the natural process of bone breakdown and repair.
Remember, most women lose about 10% of their bone in the 10 years around menopause, with the most loss taking place a year before menopause and the two years after that count most. Hot flashes and night sweats, weight gain, fuzzy thinking and fatigue are all clues that your hormones have started to shift, even years before your periods actually stop.
Carolyn J. Crandall, Aaron Aragaki, Jane A. Cauley, JoAnn E. Manson, Erin LeBlanc, Robert Wallace, Jean Wactawski-Wende, Andrea LaCroix, Mary Jo O’Sullivan, Mara Vitolins and Nelson B. Watts. Associations of Menopausal Vasomotor Symptoms with Fracture Incidence. Journal of Clinical Endocrinology & Metabolism, December 2014
Wouldn’t it be remarkable to have one way to predict future hip fracture risk?
Now, thanks to curious Finnish researchers, we have not just one, but three simple tests that can give us better insight into who is likely to break their hip down the road. After some study they settled on three physical tests, failure of which they thought might indicate that one was headed for a hip fracture. According to their findings presented at the recent ASBMR meeting, the highly predictive tests were:
Researchers had 2,791 women with the average age of 59 complete the tests — and then patiently waited 15 years to see who broke their hips.
What Researchers Discovered
Fifteen years later, researchers compared the rate of hip fracture from those women passing all tests to those women who had failed one or more of the tests. Here’s what they discovered:
• Women at age 59 failing any one of these tests had four times the risk for hip fracture, plus any fracture and even death.
• The strongest single determinant for hip fracture risk was the inability to stand on one leg for 10 seconds. In the study, failing this test at age 59 was associated with over eight times increase in hip fracture risk over the next 15 years.
• The inability to squat, touch the floor and stand back up was linked to a 5.2 times increase in hip fracture.
• Those with lowest grip strength at age 59 (or the bottom ¼ of women tested) ended up with over a four-fold increase in hip fracture as compared to women who passed the balance and squatting tests and were in the top ¾ of those tested.
What Does This Mean for You?
I’m encouraged that this research focuses on activities which suggest general fitness —and they are ones we can all practice to help minimize hip fracture risk. I suggest all women consider the following:
1. Balance is of utmost importance, if you do not fall you will not fracture a hip. If you can’t stand on one leg for 10 seconds at any age, I recommend look into exercise to enhance balance. For balance, I favor mindful exercises like Tai Chi and Qi Gong.
2. Leg strength and flexibility are hip-protective. Develop a leg strengthening exercise program. And the next time you are sitting on the floor or squatting, practice getting without using your hands. Full body strength can be enhanced with my Exercising for Bone Health DVD or the Skeletal Fitness DVD.
3. Diminished grip strength is repeatedly associated with vertebral fracture risk, and now we see it linked to hip fracture as well. If those jars are getting hard to open, it’s time to exercise your arms and hands. I like using the isometric OsteoBall exerciser to enhance arm and wrist strength.
For more information about exercise and bone health, read my article here.
Reference:
Rikkonen, T. (Sept. 12, 2014) Simple functional tests predict hip fracture and mortality in postmenopausal women: 15 year follow-up. ASBMR abstract FRO455, ASBMR Annual Meeting.





 Awhile back I told you about early research connecting menopausal hot flashes to lower bone density and a higher rate of bone breakdown. These findings from Dr. Carolyn Crandall, MD made a lot of sense to me, especially given the inflammatory nature of both hot flashes and osteoporosis.
Awhile back I told you about early research connecting menopausal hot flashes to lower bone density and a higher rate of bone breakdown. These findings from Dr. Carolyn Crandall, MD made a lot of sense to me, especially given the inflammatory nature of both hot flashes and osteoporosis.
